


Credit: Getty



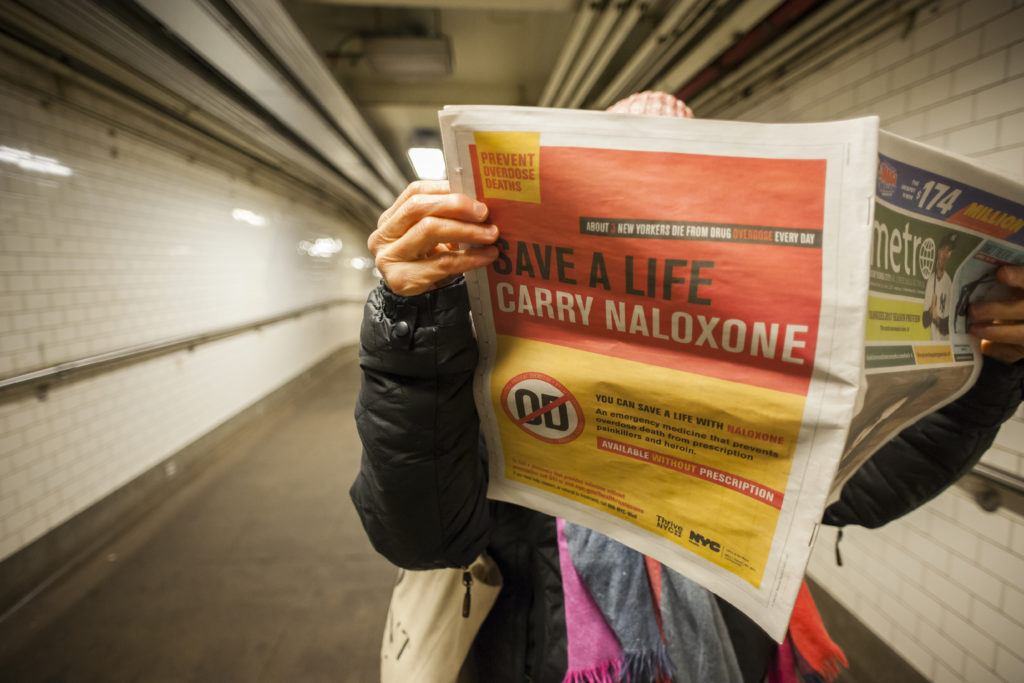
In America, almost 100 people are dying from opioids every day.
Some experts predict that half a million more people will die over the next decade . Others think it will be closer to 650,0001 – the population of Miami, or Atlanta, or Sacramento. President Trump has rightly declared the crisis a “public health emergency”.
Last week Trump’s commission on ‘Combatting Drug Addiction and the Opioid Crisis’ published its recommendations. The report has had a lukewarm reception, not least as the question of funding remains unanswered. Yet much of what it does say – from cracking down on the illegal importation of opioids to expanding drug courts and removing barriers to treatment – is sensible (we’ll park the report’s proposal for a ‘just say no’ media campaign for now).
The problem with the report lies in what it doesn’t say. Because while it traces the role of big pharma in the development of the opioid epidemic, and it seeks greater oversight of prescribing, it fails to adequately link the two. In reality, the financial relationship between pharmaceutical companies and doctors is killing people.
Like big tobacco before, big pharma is being called to account
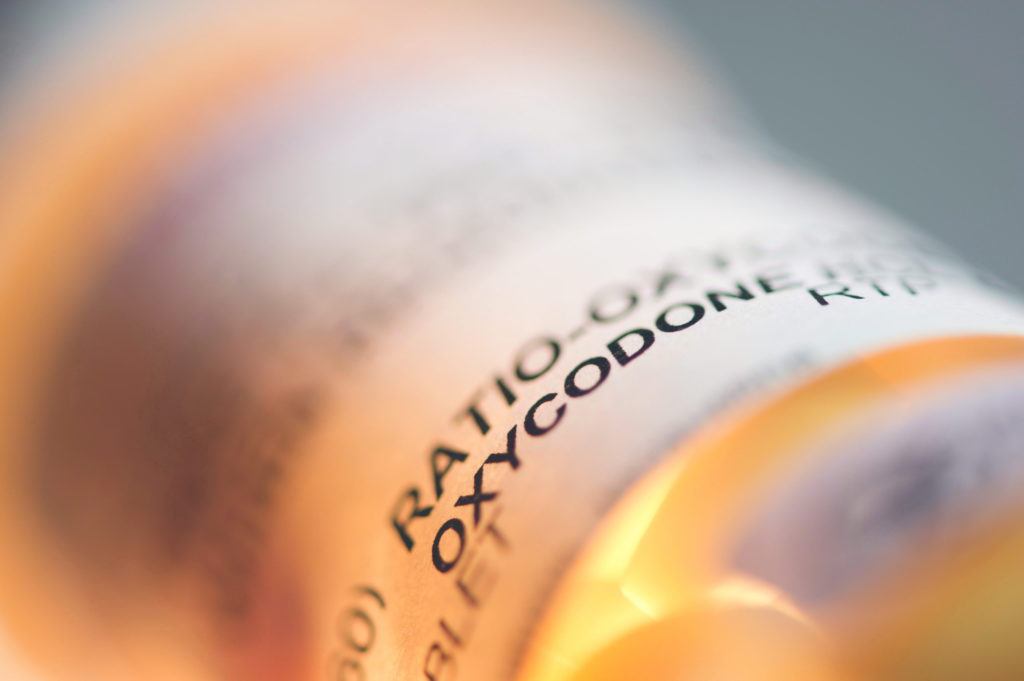
The opioid epidemic can be traced back to false advertising by big pharma in the 1990s, who peddled opioid-based painkillers as having lower risk of addiction than existing pain pills.2 More specifically, Purdue Pharma executives gave false information about their narcotic OxyContin, and doctors duly prescribed it – between 1996 and 2001 annual prescriptions increased almost 20-fold.3 Over that period, OxyContin made Purdue Pharma almost $2.8 billion.4
In 2007, Purdue Pharma finally agreed to pay $634.5 million in fines for those misleading claims, and three top executives pleaded guilty to criminal charges. 41 states are now suing the producers and distributors of opioid painkillers,5 reminiscent of the mass litigation against tobacco companies. If these companies are also found to have made misleading claims, to have behaved negligently in doling out obscene volumes of highly-addictive pills (Vox reports that enough pills were prescribed in 2016 to almost fill a bottle for every US adult), massive settlements will follow.
But as the lawsuits snowball, there’s a danger we’re missing a longer-term opportunity to protect patients.
Join the discussion
Join like minded readers that support our journalism by becoming a paid subscriber
To join the discussion in the comments, become a paid subscriber.
Join like minded readers that support our journalism, read unlimited articles and enjoy other subscriber-only benefits.
SubscribeI do cast blame for alarmist reporting. As long ago as January, we had the Diamond Princess cruise ship Covid-19 outbreak to examine. It provided some of the best early data and was clearly a worst case scenario, given the nature of cruise ships and their passengers. Prof. Michael Levitt (Nobel Chemistry 2012) looked at the numbers and concluded that the panic was overdone. Yet the press pushed the doom scenario.
Instead of a focussed approach protecting care homes etc. We did an unfocussed general lockdown, whose consequences we will have to live with for years. The devastation caused by this response (including excess mortalities) will dwarf anything purportedly saved by the panicked lockdown.
I am starting to see the data suggests Levitt was on the right track and we should make sure that is not forgotten
I can, though, sympathise a bit with the politicians for overreacting in face of the pressure put on then, not least, by vocal members of the scientific community.
A repeat though as is being suggested here and is more commonly seen as an implied threat I find negligent without taking into account the more recent data and the evidence from different approaches
I have known Michael Levitt for 40 years, I would trust his insights over the mediocre modellers who do not have the common sense to do elementary checks on their calculations.
There is a bit too much “the computer said so” in people’s thinking. How do you know it is programmed correctly? And even if the programme is good, how do you know you have entered the data correctly? If you don’t understand your model well enough to be able to do some back-of-the-envelope plausibility checks, you will never be able to trust the detailed results.
I am inherently skeptical of predictive models as even if their assumptions are okay, the errors undermine the predictive quality….you can see this when the confidence levels are included
I see some many of the assumptions being the same as those made at the pandemics start when we now have more data available and we can draw better conclusions but the dogma seems to be set.
Levitt actually kept his head and focused on the data – a lesson for us all I think
I spent about half my career ‘modeling’ and data analysis. When models produce poor predictions, it is not generally ‘errors’, although that can happen, it is that the model corresponds poorly to reality, misses something important, etc. If you want to predict Newtonian flow through a circular pipe, the equations are pretty simple, and correspond very well to reality. A computer is not needed, the equations can be solved analytically. And, the predictions correspond exactly to reality. Even a more complicated flow, can be predicted very accurately.
It’s when the model is not close to reality that the predictions are unreliable. Generally, the most common error is that some important factor is not included.
I didn’t make a detailed study, but from what I’ve read about the Imperial College ‘model’ made me laugh. It was so simplistic, it could have been a secondary school project. The fact that the predictions were wildly off the mark, could have been ‘predicted’ with a high degree of certainty.
Agree. There was much evidence to suggest a change of tack was required in April. The data was showing those most at risk and those not at risk and a report done by Holland’s public health on children and schools was in the hands of SAGE. The response could have been tailored then. Had the lockdown had been lifted for certain groups the media reaction can only be imagined. There is evidence to suggest the infection peak was before the lockdown. Some simple (and quite rough) arithmetic on incubation and length of hospital stay working back from the death peak on 11th April would seem to support this.
One thing that I still have not seen a good explanation for is the mortality peak in March/April. Was it linked to huge amount of cases (anecdotally lots of people seem to have been subject to a particularly harsh ‘flu’ in Jan/Feb)? Was it linked into leaking into hospitals and care homes and infecting people there, poor treatments, policy decisions?
We have not really seen repeats of those peaks since then and surely there must be a requirement to understand what actually happened to inform our future actions
It is a good article but then it came to saying “Better to lock down even at considerable economic cost and wait for that,” and with that I have a real issue.
We have no real data that says that a hugely damaging total lockdown is the most effective way to deal with this pandemic. It is not the same es promoting distancing, masks etc which have limited detrimental consequences.
I can accept it as an immediate reaction to the initial virus wave but to do it again with no proper assessment would be tantamount to negligence.
Would a doctor advocate administer a harsh or pharmaceutical intervention when a much milder one will have similar outcomes? Or worse administer a drug with no assessment of the benefits/risks?
Economic damage and public health are so closely intertwined that we shouldn’t underestimate consequences of a hard lockdown
I think the *soft measures*… wearing masks, and the *nana says * stuff (cover your mouth when you cough, wash your hands properly etc) and distancing will remain now in very many people, which will help, and make it interesting to see what if any effects it has on the annual influemza toll next winter.
But I agree that *lockingdown again* will be exponentially more harmful to the economy than even this first 3 months plus has been, and that has pretty disaterous, with many destroyed companies and job losses still to come throughout the rest of this year.
I just have the commonsense type view that most people I know in my ordinary life share, that we know more now than we did in March, mistakes in dealing with it were inevitable..and remain inevitable…but they should now be far smaller mistakes from here on in…and another mass lockdown would be a mega sized mistake.
Much of the damage that influenzas and coronaviruses do to our bodies is not caused directly by the virus but by our body’s first line responses attempting to slow it, before the pathogen-specific responses ramp up to clear it. Sometimes this first line system overreacts to a lethal degree.
I think the lockdown policy should be viewed in this light. A society destroying overreaction. If the economy were not already going through a huge transformation in patterns of employment, a “V” bounce back would have been possible. However the two together has accelerated the labour-shedding.
Merely printing money and trying to restore the status quo ante will not work. Worse, it may prolong the agony by inhibiting the adjustments that are needed for the new way of working.
“The big hope .. a vaccine that works .. then we’ll all be set free.” I agree, Tom. But we already have a vaccine. Tested, effective, safe. And ignored.
A vaccine raises a mild form of the disease in most, and an unpleasant case in a few. Just like covid does – but with it, the few is unacceptably too many.
However, we do know who they are. They have a biological marker, called age.
Makes it easy to spot us, and hard for us to evade capture. So round us up, keep us separate; keep us safe, keep us happy, fed, warm, entertained. Give us a good time on the rest of you, a seniors-only staycation
The rest of you kids under 55 – get infected ASAP. Back to work and play, no mask. And you know what? Most of you won’t notice if you get it.
This plan would cost millions. But after about six weeks – it’s all over! Herd immunity, or close enough for Cummings, anyway.
Present policies, of course, cost trillions. And as Tom says, deliver nothing other than delay.
But that is all too mercenary, and ignores the side-benefits from destroying our society and security. Fewer carbon emissions; that’s really important. Pass me the sick bag, can you? Mustn’t waste anything.
At this point, I take any “tell all” book written about Trump with a grain of salt. While Mary will be celebrated as a hero for her “bravery” in divulging salacious family details, the only thing it achieve is to temporarily quell the ravenous appetite of a certain segment of the population who will devour anything if it means tearing down their political boogeyman, facts, corroboration, good faith, and family intimacy be damned. Not to mention add a few zeroes to Mary’s bank account.
Mishra is like a much better-read version of Justin Trudeau. He looks all around the world today, and the most admirable government he sees, is the People’s Republic of China’s. Unbelievable!
Have people in the Anglosphere really been brought up to ignore the contributions of Germany and other countries to civilization. I still remember from my Ontario high school classes that Bismarck was arguably the greatest politician of the 19th century and the father of the modern welfare state.
In a long paper like Mishra’s that covers much of world history over centuries, virtually anyone who isn’t a professional historian is not going to be able to spot an error in most of what he says. However, when he writes that in America “welfare was turned into a dirty word by Reagan’s dog-whistles about ‘welfare queens'”, the use of “dog-whistle” genuflects to the disinformation that Reagan had invented a black welfare queen who drove around in a Cadillac to spice up his attacks on welfare abuse. In fact, Reagan got the phrase “welfare queen” and the details on the woman involved from the Chicago Tribune. Linda Taylor was a white woman, or at least that’s what her Census records said. She could change her race, as well as her age and her name, whenever she saw some advantage in it. And she did drive, at one and the same time, a Cadillac, a Lincoln, and a Chevrolet station wagon. How could this not be considered the most unconscionable kind of welfare abuse? When I read this I lost all confidence in Mishra. He’s not a reliable source of information.
Nasty article about a nasty book.
“She is suffocated by that name” -sure -choking all the way to the bank I imagine.
Firstly Correct name is SARS2 not covid 19 which is patented by Bill gates of hell,which tried with Matt hancock ,half hour to Make Certificate of Vaccination=Covid At £20 , Compulsory for Majority of 3 billion people! the Government realised it IS a Vote loser,some mandarins still dont think so. I prefer Calm approach of Oxford Professor Sunetra Gupta, and Dr Karol sikora, the 1918 Flu is still around ,less virulent now!! I HATE the hysteria foisted on US ordinary folk, whether its Brexit, Russian interference in SNP referendum ,or SARS2
Am very grateful to the writer of this article as I was getting very depressed at the idea that vaccines would not work at all. We have been promised so many things by this government eg UK app that works, world beating Track & Trace and also being told lies/misrepresentations about number of tests & ppe.#etc. Some contracts need to be examined .