






October 2, 2020 - 11:27am
Earlier this week I wrote about what appears to be a fall in the fatality rate from Covid. Part of the reason for the fall, I wrote, was that treatments for patients have improved. I listed a few — proning, use of anticoagulants, dexamethasone.
A few people, though, asked me why I hadn’t mentioned vitamin D. They seemed quite excited about it; a few even DMed me on Twitter, or emailed me, which is unusually high-effort for people replying to pieces I’ve written.
Vitamin D has been mooted for a long time as a treatment, or more accurately a prophylactic, for Covid-19. The former Brexit secretary David Davis was tweeting about it in May and July, calling for the British government to do “what Sweden, Finland and the USA do and fortify flour and milk with vitamin D to help protect the most vulnerable”. A report commissioned by Sir Patrick Vallance in July recommended its use.
But it’s been back in the news lately after a study was published in the journal PLOS One last week. “Vitamin D ‘cuts chance of coronavirus death by half’, study finds’, said the Evening Standard.
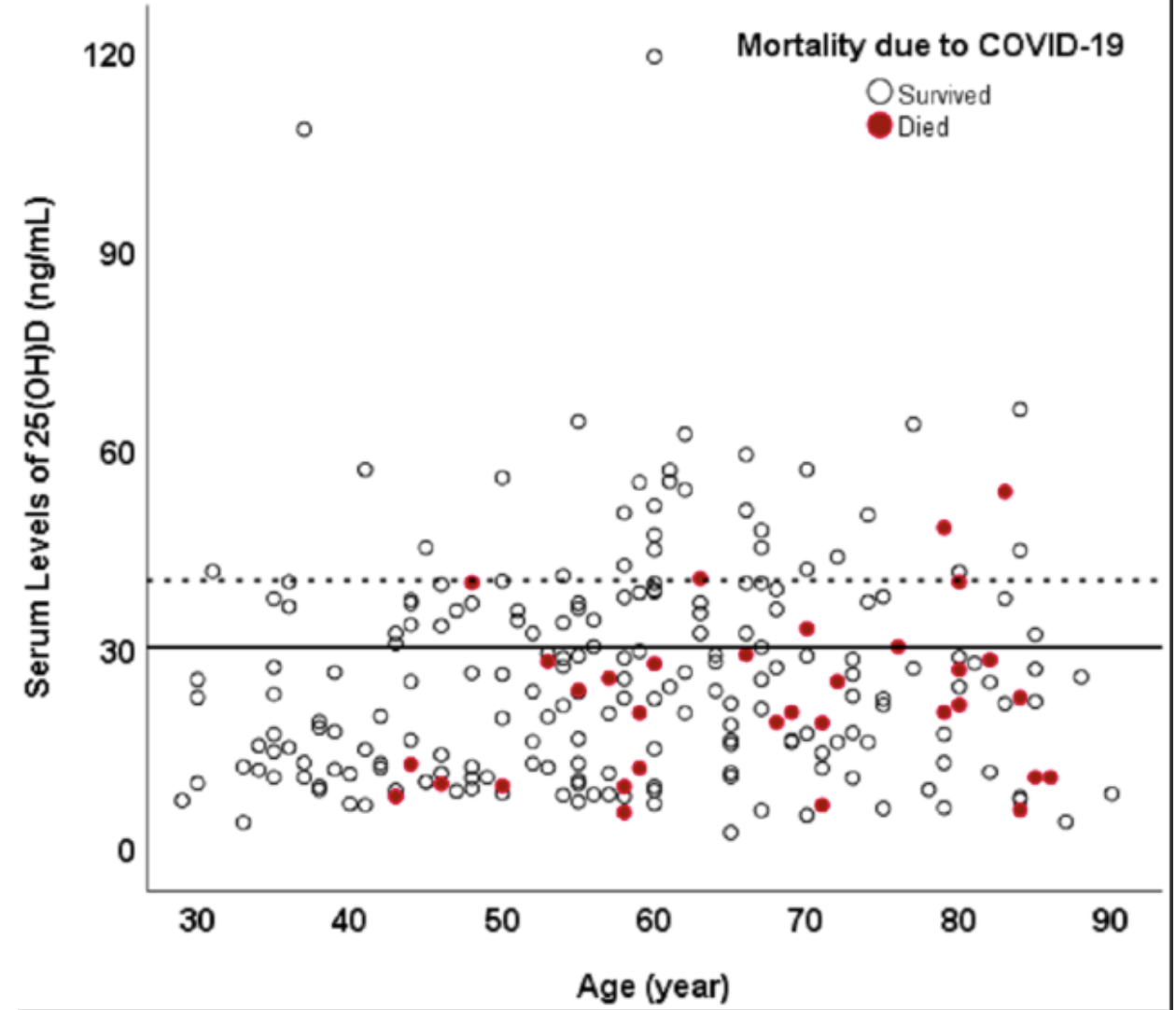
That study found, according to its abstract, that among patients over 40 who had normal levels vitamin D in their bloodstream, 9.7% died; of those who had low levels, 20% died. Which seems, on the face of it, pretty conclusive.
But it’s not a study that I would put much weight on. For one thing, it had a very small sample size — it looked at 611 patients, but as one epidemiologist has pointed out, vitamin D status was only recorded for 235 of them, and the study looked at just 150 of those. Only 34 people appear to have died, so you’re really only looking at an effective sample size of 34.

Join the discussion
Join like minded readers that support our journalism by becoming a paid subscriber
To join the discussion in the comments, become a paid subscriber.
Join like minded readers that support our journalism, read unlimited articles and enjoy other subscriber-only benefits.
SubscribeEveryone’s chemistry and biology is different.
For some it won’t work, for some it will. Like most vaccines.
The key I think is the starting point.
The levels needed are indicated for Bone health, not immune system health. Thus are too low, and the reason some countries have gone for fortification in food.
As I understand It, when the immune system is activated and Tcells are deployed, the Tcell first needs a VitD molecule to begin the fight. It’s a very good idea to have the stores full.
CDCs Dr Fauci takes 6000 IUs a day btw.
Long time reader first time poster, and usually in agreement with the author.
But I post to disagree on this one. Wrt VitD deficiency (in general), and Covid (in particular), there is a blind spot, shared with lots of rational people. The problems with this article, and in general, are:
1) Thinking as if RCT is the only source of knowledge. It is not, it is not even particularly strong knowledge, being statistical. It is prominent only because we are much ignorant (in the domains RCT is used), of very complicated things, that we have to fallback to statistical knowledge. Reasoning from 1st principles, by logic, by analogy, from observations, where possible (e.g physics/envy), is much preferred. Alas, not possible in many domains, where processes are complicated and or we know only little. So we fallback to counting the outcomes, as being the 2nd best method (and still preferred to complete agnosticism). Effectively – modelling our ignorance. [1]
2) Behaving as if “Absence of evidence is evidence of absence”. NICE expects RCT of good quality (fine), but the fact that we lack one, should not lead is to conclude “nothing to see here, move on”. On the contrary, should spur PHE, NICE etc to encourage and organize a better RCT and collect evidence. This is warranted, given the prior knowledge, observational studies, existing RCT, even before taking into account our current predicament (the pandemic). [2]
3) Being squeezed between the crazies (=cranks oblivious to any and all evidence), and IYI-s (=intellectuals-yet-idios; rational people blind to their own biases and forecasting errors, ever self-confident, suffering no ill-consequences/feedback when wrong) does not help, and makes drilling to the truth more an uphill struggle, than it objectively should be. For we have prior knowledge, plenty of data, and even the cost of errors (=taking VitD if useless v.s not taking VitD if useful) is well known.
Tom is in position of some power, and many stand to benefit if we get to the truth (whichever way it goes). Hence this comment to nudge him to keep track, and update as new evidence emerges. Few links, for- and against- the thesis “we should have sufficient VitD as not to be deficient in the midst of a global pandemic”.
https://vitamin-d-covid.sho…
https://blog.shotwell.ca/po…
https://berthub.eu/articles…
Discussions:
https://news.ycombinator.co…
https://news.ycombinator.co…
https://news.ycombinator.co…
[1] Background on good decision making using all available evidence and taking into account the cost of errors.
https://threadreaderapp.com…
https://blog.shotwell.ca/po…
[2] Latest on NICE. TLDR: NICE expects good RCT, does not accept the Spanish one.
http://www.drdavidgrimes.co…
Historically, “must RCT” criterion would have disqualified interventions on smoking and cancer, alcohol and driving, thyroid replacement, type 1 diabetes etc.
Good (satirical?) take on the “RCT is our one and only god, and we shall have none other” dogma is the BMJ’s “Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial” paper:
https://www.bmj.com/content…